OSTEOGENESIS IMPERFECTA IN A PEDIATRIC SURGICAL CENTER IN DAKAR, SENEGAL: CLINICAL AND RADIOLOGICAL ASPECTS
*Ndour O
Alumeti DM
Fall M
Faye Fall AL,
Diouf C
Ndoye A
Ngom G
Ndoye M
E-mail : roundrouma@yahoo.fr
Grant support: None
Conflict of Interest: None
Abstract
Introduction: Osteogenesis imperfecta presents with a set of constitutional disorders of varying severity, genetically determined and characterized by an abnormal production of collagen and matrix of the bone leading to bone fragility responsible for multiple fractures and many skeletal deformities. The aim of our study was to analyze the clinical and radiological aspects of the pathology.
Patients and Methods: This was a retrospective study of 10 cases of children with osteogenesis imperfecta who consulted the Pediatric Surgery Unit of the University Center Aristide Le Dantec Hospital over a period of 6 years. The parameters analyzed were the reasons for consultation, physical examination findings and findings on standard radiographs. After collecting all the data, children were divided according to the classification of Silence and Glorieux.
Results: Pain was the reason for consultation in eight children. The saber blade deformity of the legs was found in nine children. Physical examination found tenderness in 80% of cases. Blue sclera was found in one child. The teeth were normal in eight patients. Standard radiographs showed an osteopenic skeleton with multiple fractures (3.7 fractures on the average) associated with vicious callus formation and deformity. According to the classification of Silence and Glorieux, six children were type VI, two children type IV, a child type III and one type I.
Conclusion: Osteogenesis imperfecta is a rare disease. In our environment, the diagnosis is made late - a stage associated with deformity. Of these, the occurrence of sabber deformity of the lower limbs is the most common. Radiological aspects are dominated by vicious callus formation, deformed bones and osteopenia. Moderate forms are predominant. Parents need to be educated about the risk of repeat fractures and the need to present deformed children to hospital early.
Key words: Osteogenesis imperfecta, Deformities, Late diagnosis, Moderate forms, Dakar, Senegal.
REFERENCES
- Rauch F, Glorieux FH. Osteogenesis imperfecta. Lancet 2004; 363(9418) : 1377-85.
- Forin V. Ostéogenèse imparfaite et biphosphonates. Archives de pédiatrie 2005 ; 12 : 688-90.
- Bouguerra L, Turki R, Tebib M, Dahiri L. Ostéogenèse imparfaite à propos dune observation. Maghreb Médical 1995 ; 296 : 947-52.
- Fassier F. avec la collaboration de Glorieux FH. Ostéogenèse imparfaite chez lenfant. Cahiers denseignement de la SOFCOT 1999 ; 70 : 235-52.
- Thimou A, Elkarim L, MDaghri Elalaoui A, Hamdani S, Bouazzaoui Lamdaouar N. Lostéogenèse imparfaite congénitale. Maghreb Médical 1997; 316 : 47-50.
- Janus GJ, Finolori G, Engelbert RH, Pouliquen M, Pruijs JE. Operative treatment of severe scoliosis in osteogenesis imperfecta: results of 20 patients after halo traction and posterior spondylodesis with instrumentation. Eur Spine J 2000; 9: 486-91.
- Ogilvie Harris DJ, Khazim R, Beighton G. Tendon and ligament injuries in adults with osteogenesis imperfecta. J Bone Surg 1995; 77: 155-156.
- Lund AM, Muller J, Skovby F. Anthropometry of patients with osteogenesis imperfecta. Arch Dis Child 1999; 80: 542-8.
- Kuurila K, Grenman R. Response to « is it necessary to screen for hearing loss in the pediatric population with osteogenesis imperfecta? » Clin Otolaryngol Allied Sci. 2004; 29(3): 287.
- Glorieux FH, Rauch F, Plotkin H. Type V osteogenesis imperfecta: A new form of brittle bone disease. J Bone Miner Res 2000; 15(9): 1650-8.
- Minch CM, Kruse RW. Osteogenesis imperfecta: a review of basic science and diagnosis. Orthopedics 1998; 21(5): 558-67.
- Soua H, Karboul L, Ayadi A, Sassi N, Hamza N, Padovani JP, Sfarm T, Maroteaux P. Ostéogenèse imparfaite avec cal hypertrophique : à propos de deux observations à début précoce. Arch Fv Pédiatr 1993 : 47-50.
FIGURES
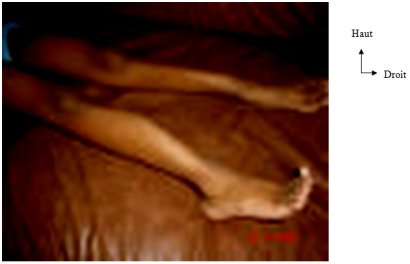
Figure 1 : Two curved saber legs (tibia)
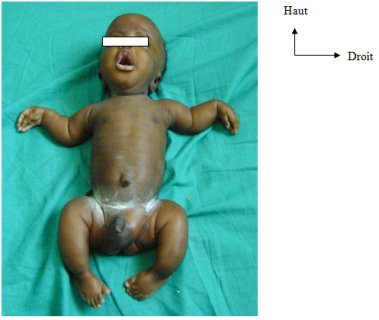
Figure 2 : Déformations multiples chez un nouveau-+
Multiple deformities ina newborn with osteogenesis imperfecta: deformity of both upper and lower limbs
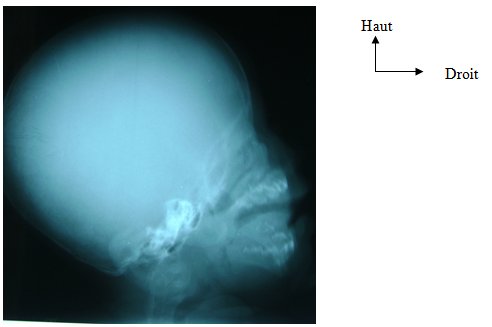
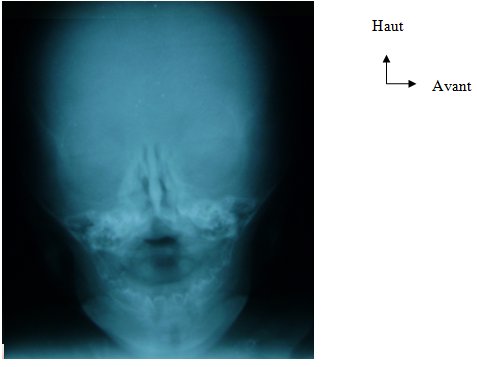
Fig. 3 and 4 : Skull x-rays showing mineralization defect of the skull
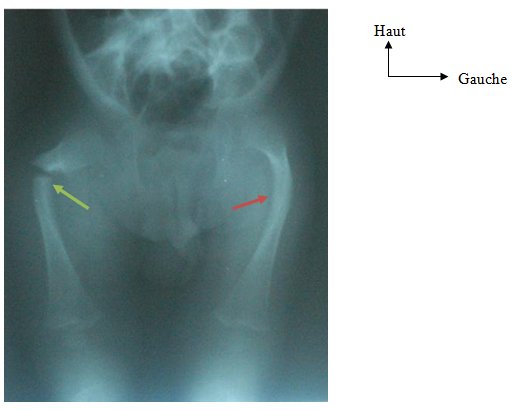
Figure 5 : X-rays of pelvis and femur showing fractures of right and left femur and left femur
| Table I : Classification of osteogenesis imperfecta of Silence and Glorieux (OI) |
|
1.
Ostéogène imparfaite de type I (bénigne) : Fractures par suite de
traumatismes minimes, sclérotique bleutée, malformation minime des os longs,
taille normale ou quasi-normale, possibilité de dentinogenèse
imparfaite. |
|
2. Ostéogène imparfaite de type II (mortelle) : Fractures intra-utérines, chapelet costal, sclérotique
bleutée, fémur large et court, détresse respiratoire, décès pendant la
période périnatale. |
|
3. Ostéogène imparfaite de type III (grave) : Fractures fréquentes par suite de traumatismes minimes,
sclérotique de couleur variable, taille extrêmement petite, grave
malformation des membres, scoliose, faciès triangulaire, dentinogenèse
imparfaite fréquente |
|
4. Ostéogène imparfaite de type IV (modérée) : Fractures par suite de traumatismes minimes, sclérotique de
couleur variable, taille modérément petite, malformation modérée des membres,
scoliose, possibilité de dentinogenèse imparfaite |
|
5. Ostéogène imparfaite de type V : Fractures par suite de traumatismes minimes, sclérotique
normale ou
légèrement bleutée, calcification de la membrane
interosseuse de lavant-bras ou de la jambe, bande métaphysaire dense sous la
plaque de croissance, callogenèse hypertrophique
par suite de fractures ou de bâtonnets intramédullaires, absence de dentinogenèse imparfaite |
|
6.
Ostéogène imparfaite de type
VI : Fractures par suite de traumatismes bénins, sclérotique
normale ou
légèrement bleutée, élévation modérée du taux de
phosphatase alcaline, stries de Looser (pseudofractures)
visibles à la radiographie, absence de dentinogenèse
imparfaite, absence dos wormiens, Absence de rachitisme. |
|
7. Ostéogène imparfaite de type VII : Fractures par suite de traumatismes bénins, sclérotique
normale ou
légèrement bleutée, absence de dentinogenèse
imparfaite, coxa vara, rhizomélie (brièveté des
racines des membres supérieurs et inférieurs) |
| Table II : Details of the patients |
|
Nom/Prénom |
Sexe |
Age |
Poids/Taille |
Déviations standard |
|
B.B G.M D.I S.D K.S K.Z S.I D.S D.A L.M |
Masculin Masculin Masculin Masculin Masculin Masculin Masculin Masculin Féminin Féminin |
15 ans 11 ans 8 ans 5 ans 1 an 5 mois 8 mois 2 mois 15 jours 15 jours 10 jours |
37 Kg/140 cm 11 Kg/85 cm 16 Kg/106 cm 11 Kg/97 cm 8 Kg/70 cm 5,58 Kg/59 cm 4,5 Kg/55 cm 2,5 Kg/50 cm 3 Kg/51 cm 2,5 Kg/45 cm |
-2DS/-3DS -3DS/-3DS -2DS/-3DS -3DS/-2DS -1DS/-3DS -1DS/-3DS Normal Normal Normal Normal |