PATTERN OF HAND INJURIES IN OSOGBO, SOUTH-WEST NIGERIA
Olaitan P.B1., Oseni G.O1., Olakulehin O.A2
Burn and Plastic surgery Unit, Orthopaedic Unit, Department of Surgery, Ladoke Akintola University of Technology Teaching Hospital, Osogbo, Osun State, Nigeria.
E-mail: emiolaitan@yahoomail.com
*CorrespondenceGrant support: None
Conflict of Interest: None
ABSTRACT
BACKGROUND: Injury to the hand leads to loss of function with attendant psychological consequences. Epidemiological studies of hand injuries from our environment are few; hence the need for this study.
AIMS AND OBJECTIVES: To assess the epidemiology of hand injuries with a view to suggesting some methods of preventing the injuries in our environment.
SETTING: This study was carried out in a Plastic surgery unit of a teaching hospital in Nigeria.
METHODS: A retrospective review of the epidemiology of hand injuries in Osogbo, Nigeria was done. Sources of information include the case notes and operating registers. Information obtained includes biodata, aetiologies, pattern of injuries, presentation, treatment as well as complications.
RESULTS: A total of 74 patients with hand injuries were managed during the study period comprising of 53 males and 21 females. The age group 21-30 was the most affected. Students form the largest group affected with 24(32.4%) followed by artisans, 16 (21.6%). The most common source of hand injuries was road traffic crash with 29 (39.2%) patients. Others were Blast injuries, 2 (2.8%), avulsion from grinding machines, 10 (13.5%), other domestic accidents, 6 (8.2%), broken bottles, 4 (5.4%), glass cut, 4 (5.4%), farm accidents, 6 (8.2%), electrical burns, 4 (5.4%), gunshot injuries, 3 (4.0%), thermal burns, 6 (8.1%) and constricting ring, 4 (5.4%).
Injuries involved only the right hand in 36 (48.6%) patients, the left, 28 (37.8%) patients and both hands, 10 (13.5%) patients. Anatomical disruptions observed included avulsion, 14 (18.9%) patients, burn, 6 (8.1%)patients, bruises, 2 (2.7%) patients, crush injuries, 13 (17.6%), laceration, 24(33.8%), fractures/dislocation, 14(18,9%), and digital gangrene, 1(1.4%) patient.CONCLUSION: Hand injury prevention will include provision of safe road and education of the people on the use of tools and machines in our environment.
Key words: Epidemiology, Hand injuries, Prevention, Nigeria.
Introduction
The hand is a very important part of the body used for exploratory and manipulatory activities. It is the organ involved in prehension. Hands play an important role in maintaining body image and sense of identity as well as serving as an organ of communication among other things. Hands often get injured and thereby incapacitating the patient if proper care is not given. Injury to the hand leads to loss of function as well as deformity of body image which has a lot of psychological consequences. These injuries can arise from different ways and the knowledge of these is important not only to plan for the treatment but also to plan injury preventive methods. Epidemiology of the hand injury may vary from one community to another depending on the occupation and industrial activities in that location. Preventive methods for hand injuries depend on the epidemiology of the injuries in the particular environment. We present a review of the epidemiology of hand injuries presenting to an emergency unit of a developing country. In our environment, most patients pay for their treatment. Treatment may therefore suffer where funds are not immediately available to the patients. The current study is set out to identify the aetiologies of hand injuries, presentation, treatment, and then offer suggestions on possible prevention protocol.
Materials and Methods
This was a retrospective review of patients who presented and were managed for hand injuries at the Accident and Emergency Unit of Ladoke Akintola University of Technology Teaching Hospital, Osogbo, Nigeria between April 2006 and April 2010. The admission and operation registers as well as case notes of patients treated at the unit were the sources of the information. Information obtained include patients biodata, handedness, occupation, aetiology and type of the injuries, hand involved whether right or left as well as part(s) of the hand involved, management given as well as the results were documented. The results were analysed using mean, frequencies and student t test.
Results
A total of 74 patients with hand injuries were managed at our emergency unit over the study period. There were 53 males and 21 females bringing the male to female ratio to 2.5:1. The age group 21-30 was the most affected with 26 (35.1%)patients followed by 11-20 with 13 (17.6%) and 1-10 and 31-40 with 16.2% patients respectively (Fig 1). Sixty six (89.2%) of the patients were right handed while 5 (6.8%) were left handed and 3 (4.1%) of them used both hands equally.
Students were the most affected with 24(32.4%) followed by artisans, 16 (21.6%). Others were as shown in table 1.
One (1.4%) of the patients was diabetic while another one had hypertension as a medical problem.
The most common source of hand injuries was road traffic crash with 29 (39.2%) patients. Blast injuries from tear gas occurred in 2 (2.8%), avulsion injuries from grinding machines in 10 (13.5%), domestic accidents in 6 (8.2%), broken bottles in 4 (5.4%), glass cut in 4 (5.4%), farm accidents including machete cut in 6 (8.2%), electrical burns in 4 (5.4%), gunshot injuries in 3 (4.0%), others including thermal burns, constricting ring, 4 (5.4%)(Table 2).
The right hand alone was injured in 36 (48.6%) patients, the left hand in 28 (37.8%) patients and the rest 10 (13.5%)sustained injuries to both hands meaning that the right hand was the most injured, with 46 (62.2%) patients. Anatomical disruptions observed in the patients varied and included avulsion in 14 (18.9%) patients, burn in 6 (8.1%) patients, abraision 2 (2.7%) patients, crush injuries 13 (17.6%), laceration 24(33.8%), fractures/dislocation 14 (18,9%), and digital gangrene, 1(1.4%) patient. Table 3.
All the patients had wound debridement alone or in addition to other treatment modalities. While all the patients had wound debridement, nineteen (25.7%) of the patients had wound debridement alone. Other treatments offered to the patients to restore function were direct wound closure in 4 (5.4%) patients, Split thickness Skin grafting, 13 (17.6%), cross finger flap closure, 3 (4.0%), groin flap cover, 3 (4.0%), K-wire immobilisation,9 (12.2%), tendon repair, 12 (16.2%), nerve repair 4 (5.4%), refashioning of digits, 2 (2.0%), and amputation 3 (4.0%).Table 4.
Only 16 of the patients had wound swab taken for microscopy, culture and sensitivity. The growth showed Staphylococcus aureaus as the most predominant organism in 8 (50.0%) of the patients and in addition to Klebsiella in 1 patient whereas Klebsiella was cultured in 2 of the wounds alone and in addition to Pseudomonas in another wound. Pseudomonas was cultured in one of the wounds alone and Escherichian coli in another wound.
Sixty six of the patients were admitted for treatment of their injuries and their hospital stay ranged between one day to seven months with a mean of 29.8±37.58 days. Complications observed in the current study included contracture in 3 patients, infection in 5 patients and severe sepsis in a patient with underlying diabetes mellitus.
Discussion
Next to the brain, the hand is the greatest asset to man, and to it is due the development of Mans handiwork1. Hands and digits of the humans occupy a major role and is one of the organs in the body that is commonly injured2,3. Hand injuries have been reported to occur from several aetiologies4-6. Injuries of the hand have an enormous impact on hand function and on quality of life7. These injuries are as preventable as the other bodily traumas8. Knowledge of epidemiology and etiology of hand fractures9 and injuries generally serve as an essential first step in devising strategies to reduce the incidence of these hand injuries.
The most common cause of hand injuries in the current study was road traffic crash observed in 29 (39.2%) patients while occupation related injuries were observed in 22 (29.7%) patients including blast injuries from tear gas in 2 (2.8%), grinding machine in 10 (13.5%),farm accidents including matchet cut in 6 (8.2%), electrical burns in 4 (5.4%) patients.
Acute hand injury has been observed as the leading cause of occupational injury treated in United States' hospital emergency departments (e.g., laceration, crush or fracture)11. Poor road maintenance cultures as well as the use of poorly maintained vehicles are the main cause of road traffic crash in Nigeria. Other reasons may include reckless driving and poor knowledge of road signs.
A previous study has revealed a male: female ratio of 1.7:1.0 with both left and right hands being relatively equally injured12. The current study shows a male::female ratio of 2.5:1 with right hand injuries in 46 (62.2%) patients and the left in 38 (51.4%) patients. The difference was possibly ascribable to the fact that the occupations from which many of the injuries in the current study occurred were known to be commonly a male predominant setting.
The high incidence of hand injuries from road traffic crash is much different from that observed in the paediatric age group who had domestic accidents as the most common sources of hand injuries in our environemnt10. This can be explained by the fact that the adults are more likely to travel in motor vehicles in the course of their daily routine. In developed countries like Denmark and Netherlands12 hand injuries show a peak for teenagers, result mainly from home and leisure accidents and are mainly caused by objects and falls. This is different from our present study both in aetiologies as well as pattern of injuries.
It has been observed that Hand injuries can result in lengthy periods off work14. The mean period of admission of patients in the current study was 29.8±37.58 days. This is a huge time loss by the patients and economic loss in terms of productivity apart from the cost of taking care of these patients. Inability of the patients to make money available for surgical procedures needed account significantly for this.
Hand injuries are as preventable as the other bodily traumas8. Hand trauma can be prevented by providing a safer environment at home, at work and in the playground.
We conclude that hand injuries are a real burden to society and are worthwhile to be prevented with special attention for home and leisure accidents and occupational accidents.
References
- Greco R.J. Basic Evaluation of Upper Extremity Injury. In: Richard J. Greco (editor). Emergency Plastic Surgery. Boston/Toronto/London: Little Brown and Company; 1991. 59-88.
- Burke FD, Dias JJ, Lunn PG, Bradley M. Providing care for hand disorders: Trauma and elective. The Derby Hand experience (1989-90). J Hand Surg [Br] 1991; 16(1):13 8.
- Trybus M, Lorkowski J, Bronjel L, Hladki WCauses and consequences of hand injuries. The American Journal of Surgery 192; (2006) 5257.
- Benfield R, Plurad DS, Lam L, etc. The epidemiology of dog attacks in an urban environment and the risk of vascular injury. Am Surg. 2010; 76(2):203-5.
- Davidson CC, Eadie PA. Burning more calories: treadmill friction injuries in children. Ir Med J. 2009;102(10):320-3.
- Olaitan P.B., Jiburum B.C. Review of 106 hand digit amputation. Nigerian Journal of Orthopaedic and Trauma; 2008; 7(1):3-6.
- Benfield R, Plurad DS, Lam L, Talving P, Green DJ, Putty B, et al. Inaba K, Cestero R, Demetriades D. The epidemiology of dog attacks in an urban environment and the risk of vascular injury. Am Surg. 2010;76(2):203-5.
- David SS, Goel K. Knowledge, attitude, and practice of sugarcane crushers towards hand injury prevention strategies in India. Inj Prev. 2001;7(4):329-30.
- Surveillance for non-fatal occupational injuries treated in hospital emergency departmentsUnited States, 1996 (1998) MMWR Morb Mortal Wkly Rep 47, 3026.
- Mahabir RC, Kazemi AR, Cannon WG, Courtemanche DJ. pediatric hand fractures: a review. Pediatr Emerg Care. 2001;17(3):153-6.
- Olaitan P.B., Ogbonnaya IS. Hand injuries In Paediatric age group. African Journal of Paediatric Surgery. 2005; 1(2): 67-70.
- Sorock GS, Lombardi DA, Hauser RB, Eisen EA, Herrick RF, Mittleman MA. A case-crossover study of occupational traumatic hand injury: methods and initial findings. Am J Ind Med. 2001;39(2):171-9.
- Larsen CF, Mulder S, Johansen AM, Stam C. The epidemiology of hand injuries in The Netherlands and Denmark. Eur J Epidemiol. 2004;19(4):323-7.
- Kenesi C, Masmejean E. Emergency treatment of hand trauma in France, an important public health challenge. Bull Acad Natl Med. 2004;188(5):793-800.
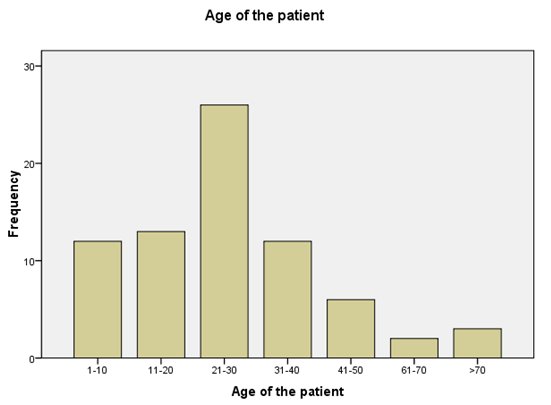
Fig 1. Age of the patients with hand injuries
| Table 1. Occupation of the patients with hand injuries |
|
Number of patients Number of patients percentage |
|
Civil
servant 8 10.8 Farming 4 5.4 Artisan 16 21.6 Schooling 11 14.9 Child 24 32.4 Driving 4 5.4 Others 5 6.8 |
|
TOTAL 74 100.0 |
| Table 2. The causes of the hand injuries |
|
Aetiology |
Frequecy |
Percentage |
|
|
Road traffic accident |
38 |
51.4 |
|
|
Burns |
7 |
9.5 |
|
|
Domestic cuts |
15 |
20.3 |
|
|
Firearms |
3 |
4.1 |
|
|
Workplace accident |
4 |
5.4 |
|
|
Farm accident |
5 |
6.8 |
|
|
Assault |
1 |
1.4 |
|
|
Not indicated |
1 |
1.4 |
|
|
Total |
74 |
100 |
|
| Table 3. Anatomical disruptions observed in patients |
|
Anatomical
disruption |
No
of patients |
Percentage |
|
Laceration |
24 |
32.4 |
|
Avulsion |
14 |
18.9 |
|
Crush injuries |
13 |
17.6 |
|
Burns |
6 |
8.1 |
|
Bruises |
2 |
2.7 |
|
Fracture/dislocation Gangrene |
14 1 |
18.9 1.4 |
|
Total |
74 |
100 |
| Table 4. Procedures performed on the Patients |
|
Procedures Number of patients Percentage |
|
Wound debridement alone 19 25.7 Direct closure 4 5.4 Skin graft 13 17.6 Cross finger flaps 3 4.0 Groin flaps 3 4.0 k-wire immobilization 9 12.0 Tendon repair 4 5.4 Nerve repair 4 5.4 Refashioning of digits 2 2.6 Amputation 3 4.0 |
|
Total 74 100. |